


THE PROBLEM
Most clinical research leave people behind
Traditional clinical research require repeated in-person visits, which shuts out people who can't travel, take time off work, or afford the burden. The result: studies that are slow, expensive, and don't reflect the real world. Additionally, the implementation of the interventions and tools in clinical care are not often studied, leading to poor workflows or reduced adoption rates in real world health systems leaving behind those asked to use and implement the interventions.
Digital tools exist. But most research still don't use them.
Smartphones, wearable devices, and home monitors already let people track their health from anywhere. If applied to research, these tools can replace clinic visits entirely. Some studies have already enrolled hundreds of thousands of people this way.
Yet fewer than 4% of trials use remote methods in any meaningful way. The infrastructure to coordinate devices, sustain engagement, and connect findings to clinical care simply doesn't exist — so most teams are left building it from scratch.
That gap, between what's possible and what's actually happening, is what UNITED is built to close.
THE PROOF
Has it been done before?
UNITED's foundation were built from UMass Chan's experience contributing to RADx, an NIH initiative aiming to speed up the development, validation, and commercialization of point-of-care and home-based tests. UMass Chan led the Clinical Studies Core and thus the design and implementation of nationwide studies that enrolled thousands of participants remotely - no clinic visits required. The findings of these studies directly informed FDA and CDC guidelines, proving that decentralized research can operate at scale and drive real policy change.
It has since been applied to a remote pulmonary rehabilitation study for patients with COPD leading to a full scale implementation in the UMass Memorial Health System for providers to refer patients to. Currently, this same methodology is powering PILLAR, a remote monitoring program for lupus. Each project adds new tools, workflows, and evidence back into the platform.
It doesn't just collect data. It turns data into discovery that informs clinical care delivery
UNITED brings together four types of information that are usually kept separate: patient surveys, wearable device readings, patient-generated media (like uploaded pictures, voice recordings), and home-collected biospecimens. Everything flows into a single secure platform that uses advanced data analysis and machine learning to surface patterns that occur between routine clinic visits and would otherwise be missed. Those insights are used to inform clinical care, so research findings don't sit in a database waiting to be published. The UNITED platform takes this one step further and studies the implementation into the clinic care workflow to improve integration and adoption of the intervention.
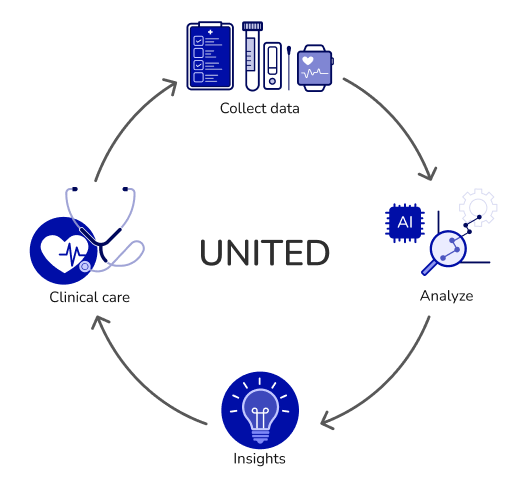
At the heart of this is the learning community: a standing group of patients, clinicians, researchers, and administrators who meet regularly to review findings and shape the program together. Evidence connects to care continuously, not years later. Moreover tools, workflows, and findings from every project would be added to an open learning library, freely available to any research team.

THE PROOF
Has it been done before?
UNITED's foundation were built from UMass Chan's experience contributing to RADx, an NIH initiative aiming to speed up the development, validation, and commercialization of point-of-care and home-based tests. UMass Chan led the Clinical Studies Core and thus the design and implementation of nationwide studies that enrolled thousands of participants remotely - no clinic visits required. The findings of these studies directly informed FDA and CDC guidelines, proving that decentralized research can operate at scale and drive real policy change.
It has since been applied to a remote pulmonary rehabilitation study for patients with COPD leading to a full scale implementation in the UMass Memorial Health System for providers to refer patients to. Currently, this same methodology is powering PILLAR, a remote monitoring program for lupus. Each project adds new tools, workflows, and evidence back into the platform.
CASE STUDY
PILLAR: Remote monitoring for lupus
PILLAR, Patient-centered Interventions for Lupus monitoring using Learning-based Adaptive Recognition, will be the first project running on the UNITED platform. It focuses on lupus, a complex autoimmune disease that disproportionately affects Black, Hispanic, and Asian women, and one where current monitoring relies almost entirely on in-person visits that many patients struggle to keep.
Using the UNITED platform, PILLAR will deliver a remote monitoring program directly into patients' daily lives — wearable devices, home blood pressure readings, symptom surveys, and self-collected biospecimens. Clinicians would receive a summary of each patient's data before appointments. The research team will simultaneously identify which outreach strategies keep patients engaged over time.
PILLAR will be both, a research study and a clinical program. Data collected by patients doesn't just feed a dataset — it informs real care decisions, in real time, within the existing workflow of the UMass Lupus Center.