

Disordered Eating
Objectives:
- Understand the clinical presentation and diagnosis of anorexia nervosa, bulimia nervosa, binge eating disorder, and avoidant/restrictive food intake disorder
- Understand the different treatment modalities for eating disorders
- Know how to reference the UMass Disordered Eating Protocol for 5E
- Consider and evaluate for differential diagnoses of disordered eating
- Understand refeeding syndrome including the underlying mechanism and how to monitor and treat
Articles:
- Eating Disorders. Ellen S. Rome, Sarah E. Strandjord. Pediatrics in Review, 2016
- Case based learning discussing Anorexia Nervosa, Bulimia Nervosa, Binge Eating Disorder, Other Specified Feeding or Eating Disorder, Avoidant/Restrictive Food Intake Disorder
- Eating Disorders in Children and Adolescents: State of the Art Review. Kenisha Campbell, Rebecka Peebles. Pediatrics, 2014
- State of the Art Review Article about Eating Disorders in Children and Adolescents
- Discusses epidemiology, etiology, clinical presentation, diagnosis, complications, treatment, prevention
- Refeeding Syndrome. , and Pediatrics in Review, 2016.
- Case examples to review refeeding syndrome.
- Practice parameter for the assessment and treatment of children and adolescents with eating disorders. Lock, J., & La Via, M. C. J Am Acad Child Adolesc Psychiatry, 2015
- American Academy of Child and Adolescent Psychiatry Committee Practice parameters
- Discusses anorexia nervosa clinical presentation and course, epidemiology, etiology and risk factors, differential diagnosis and comorbidity; bulimia nervosa clinical presentation and course, epidemiology, etiology and risk factors, differential diagnosis and comorbidity; binge eating disorder clinical presentation and course, epidemiology, etiology and risk factors, differential diagnosis and comorbidity; avoidant restrictive food intake disorder clinical presentation, epidemiology, etiology and risk factors, differential diagnosis; other specified feeding or eating disorders; evidence base for practice parameters (7 recommendations)
Additional Resources:
- Check out our UMass Resident Guide to the inpatient Disordered Eating Protocol, 2020 version
- Pediatric Care Online Chapter 216: Anorexia Nervosa, Bulimia Nervosa, and Other Eating Disorders
-
- Link to this online textbook via the Lamar Soutter Library site
- Discusses etiology, definitions, clinical manifestations, differential diagnosis, evaluation, treatment, outcome, prognosis, prevention, AAP policy, more suggested readings
- National Eating Disorders Association website
- CHOP Clinical Pathway for Evaluation and Treatment of Patients with Malnutrition, Weight Loss, and Eating Disorders
Self-Assessment:
1. A 14-year-old adolescent is brought to your office for fatigue and decreased appetite that she has experienced over the past month. She has associated nausea but no vomiting, diarrhea, or fever. Her medical history is significant for autoimmune hypothyroidism since age 8 years, for which she takes levothyroxine daily. Physical examination reveals a temperature of 37°C, heart rate of 120 beats/min, blood pressure of 90/48 mm Hg, respiratory rate of 16 breaths/min, weight of 44.6 kg (25th percentile), height of 165 cm (75th percentile), and body mass index of 16.4 kg/m2 (10th percentile). She appears tired, with diffusely hyperpigmented skin. Capillary refill time is 3 seconds. The remainder of her physical examination findings are unremarkable.
Of the following, this girl’s MOST likely diagnosis is
- adrenal insufficiency
- anemia
- anorexia nervosa
- gastroparesis
- uncontrolled hypothyroidism
2. You are seeing a 16-year-old girl in the emergency department. She was referred by her primary care provider for concerns of dehydration. Her father reports that the girl has had poor oral intake for the last 3 months, over which time she has lost 16 kg. During an interview with the girl alone, she discloses that she was very upset about her weight and placed herself on a 500 kcal/day diet 3 months ago. The girl reports that she often feels fat and bloated. She uses an over-the-counter diuretic 3 or 4 times per day. On physical examination, the girl’s body mass index is at the second percentile for age. Her heart rate is 49 beats/min and her blood pressure is 90/55 mm Hg. She has lanugo hair on her chest and marked diffuse muscle wasting.
Of the following, a diagnostic criterion for this patient’s suspected condition is
- amenorrhea
- excessive exercise
- intense fear of gaining weight
- self-induced vomiting
- use of medication to prevent weight gain
3. A 14-year-old girl is in the office for a routine follow-up visit. For the past 3 months, she has been treated for anorexia nervosa by a multidisciplinary team. Overall she is doing well with treatment and has gained 4.5 kg. Her current weight is 43.2 kg and body mass index is 15.4 kg/m2 (3rd percentile). She is working hard to eat 3 balanced meals per day and limit her exercise to no more than 1 hour/day of moderate-intensity swimming. Her last menstrual period was 6 months ago. Dual-energy X-ray absorptiometry (DXA) performed as part of a comprehensive evaluation shows low bone mineral density for age. Her mother is very concerned about this result because the girl’s grandmother died of complications after a hip fracture. She asks what can be done to improve her daughter’s bone density.
Of the following, the intervention likely to be the MOST effective is
- adequate caloric intake for continued weight gain
- increased weight-bearing activity
- replacement estrogen and progesterone
- supplemental calcium and vitamin D
4. A 17-year-old adolescent girl with anorexia nervosa is admitted to the hospital for inpatient psychiatric support and placement of nasogastric feeding tube. She has had persistent weight loss, restrictive eating behaviors, and laxative abuse, despite maximizing outpatient therapy. She describes frequent nausea and daily episodes of nonbilious nonbloody emesis. Over the last 6 months, she has lost 11 kg, and her body weight at the time of admission is 38 kg (body mass index, 14.1 kg/m2). She reports that she eats small amounts of food once or twice daily. Her last menstrual period was 6 months ago.
Laboratory data are shown.
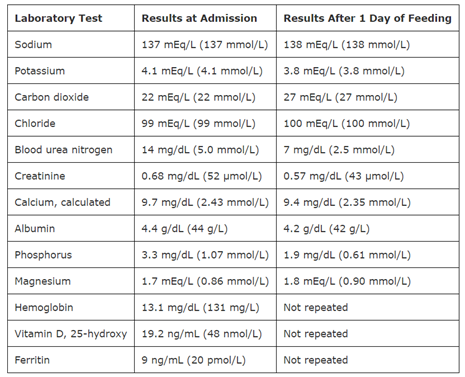
Of the following, the intervention MOST indicated in this patient is:
- intravenous iron sucrose
- intravenous potassium
- oral magnesium
- oral phosphate